Taken from American Heart Association Task Force / American College of Cardiology Guidelines 2006.
Murmur MS
The first heart sound is loud (causing a palpable tapping apex)
The second heart sound is normal
There is an opening snap in diastole heard shortly after the first heart sound
There is rumbling diastolic murmur heard most clearly with the bell of the stethoscope over the apex with the patient in the left lateral position.
There are no other added sound
Murmur is accentuated by exercise
Consider anticoagulation with warfarin due to high risk of AF.
Aortic Stenosis
Aortic STENOSIS
Gradient across the valve
Valve area (normally is over 2cm2)
Mild
<25 mm Hg
>1.3-2cm2
Mod
25-40mm Hg
0.7-1.3cm2
Severe
>40 mmHg
< 0.7cm2
Other markers
Cardiomegaly/ Impaired LV function/ Dysrhythmias
Taken from American Heart Association Task Force / American College of Cardiology Guidelines 2006.
Murmur AS
The first heart sound is normal
The second heart sound is soft (stenosed valve closes slowly)
There is a harsh ejection systolic murmur heard loudest in the aortic area that radiates to both carotids.
There are no other added sounds [there may be an ejection click in patients with a bicuspid aortic valve]
The diagnosis is most likely to be aortic stenosis
The differential would include MR however the fact the murmur has the characteristics of an ESM loudest etc makes this less likely
Aortic stenosis – causes
Degenerative calcification (Calcific AS)*
Rheumatic Heart disease
Bicuspid aortic valve – Patients can present late with symptoms
Congenital
*thought to be unrelated to cholesterol although new evidence emerging
Aortic And Mitral Regurgitation
Aortic Regurgitation
American Heart Association Task Force/ American College of Cardiology Guidelines 2006
Regurgitant fraction of cardiac output
Regurgitant Orifice size
Mild
<30%
<0.1cm2
Moderate
30-50%
0.1-0.29 cm2
Severe* *increase in LV dilatation
>50%
>0.3 cm2
Murmur AR
The first heart sound is normal
The second heart sound is normal
There is no systolic murmur
There is an early diastolic murmur heard loudest in expiration at the left sternal edge with the patient sat forwards.
There are no other added sounds [there may be an ejection click in patients with a bicuspid aortic valve]
The diagnosis is most likely to be aortic regurgitation. The differential diagnosis of a diastolic murmur includes mitral stenosis but this murmur has no features to suggest that.
Other features
Collapsing pulse.
Wide pulse pressure
Corrigan’s sign: prominent arterial pulsations in the neck
de Musset’s sign (head nodding in time with the heart beat)
Quincke’s Sign(pulsation of the capillary bed in the nail)
Traube’s sign (Pistol shot femoral pulses! A load systolic murmur is heard over the femorals as a result of the hyperdynamic circulation)
Thrusting apex (volume overloaded LV in the same was as a HOCM could do this)
American Heart Association Task Force/ American College of Cardiology Guidelines 2006
Regurgitant fraction
Regurgitant Orifice size
Mild
<30%
<0.2 cm2
Moderate
30-50%
0.2-0.39 cm2
Severe* *need LA and LV size to be increased
>50% and LV dilatation and LA dilatation
>0.4 cm2
Common Causes
Remember anything which affects either the LV size/ the valve leaflets (SBE, connective tissue disease/ age related degeneration/ chordae tendinae rupture post MI (connections to the papilliary muscle that stop the valve from prolapsing) can cause MR.
Degenerative disease
LV dilatation of any cause causing a functional MR – IHD, hypertensive heart disease
Rheumatic Heart disease
Other (SLE/ diseases of connective tissue (e.g. Marfan’s/ Ehlers Danlos/ pseudoxanthoma elasticorum, SLE)
Murmur of MR
The first heart sound is soft
The second heart sound is normal
[There may be a third heart sound/ there are no added sounds]
There is a pan systolic murmur heard loudest at the apex radiating to the axilla.
Pulmonary StenosisAmerican Heart Association Task Force/ American College of Cardiology Guidelines 2006
Criteria
Severe PS
Gradients >60mmHg across the Valve
Commonest Causes of Congenital Heart Disease
Condition
1) VSD
Initially LàR shunt that can then reverse causing an Eisenmenger’s syndrome (i.e. initially not cyanosis as oxygenated blood is being shunted from Là R. But… if this reverses then deoxygenated blood will be shunted from Rà L causing cyanosis
2) ASD
Fixed wide splitting of S2
3)Patent Ductus Arteriosus
Collapsing pulse Continuous machinery murmur (blood shunting from pulmonary artery to subclavian artery- conservative Mxàpercutaneous closure]
4) Fallot’s Tetralogy
VSD, Aorta that overrides VSD, RVH and Pulmonary stenosis. History: Blalock Shunt: pulmonary artery to the subclavian artery.
Prosthetic/ Metal Heart Valves Anticoagulate Target INR of 3.5 (3-4.5)
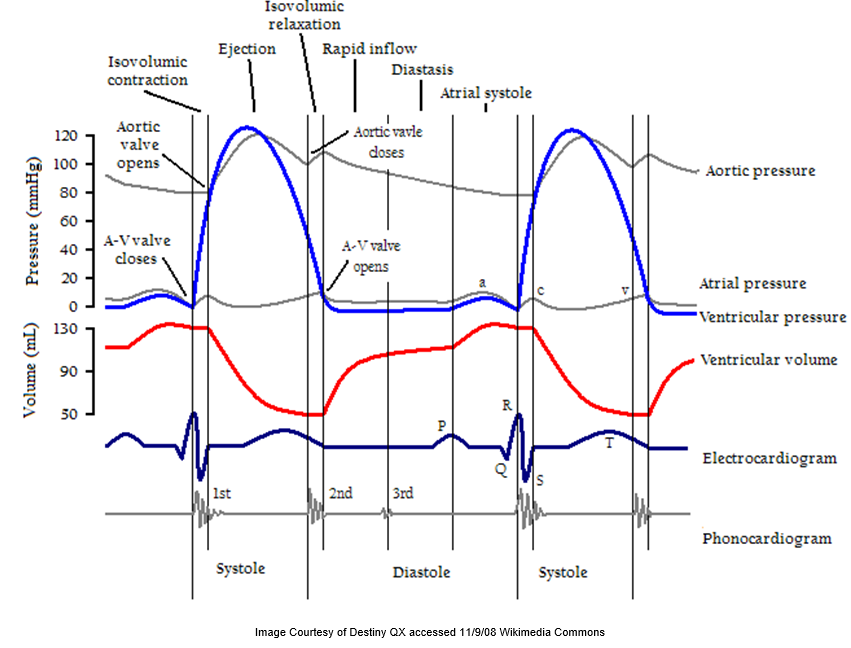
Atrial Diastole: 30ml of blood passively fills the ventricle
90ml blood in LV at end of diastole
Atrial Systole: 40ml more blood flows into the LV
130ml Blood in the LV
Ventricular Systole: approx 70ml of blood is ejected from the 130 ml in the LV. This represents the stroke volume. The ejection fraction is SV/ (SV+LV end diastolic volume ) i.e. 70/(70+60)