A suggested method is to use the American Spinal Injury Association Classification of Nerve Roots and Spinal Reflexes. This is standard and published by a reputable source to allow clear communication between clinicians and Neurosurgical units.
The ASIA Standard Neurological Classification of Spinal Cord Injury Is Shown Below
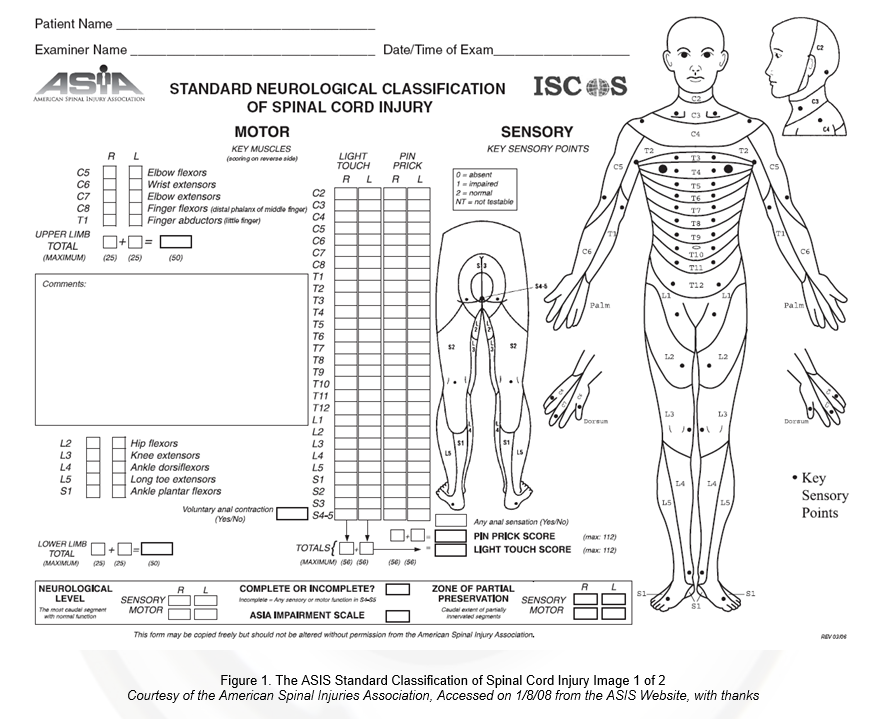
Figure 1. The ASIS Standard Classification of Spinal Cord Injury Image 1 of 2
Courtesy of the American Spinal Injuries Association, Accessed on 1/8/08 from the ASIS Website, with thanks
Inspect from the end of the bed
Inspection
- Posture
- General health
- Deformities / contractures
- Muscle wasting
- Fasciculations
- Abnormal movement – chorea etc
- Around the bed – walking aids
Tone
- Normal / reduced / increased. Unilateral / bilateral
- Cog-wheeling
- Check for clonus (UMN lesion)
- Spasticity (UMN)
Power
| MRC Grade (Medical Research Council) | Movement (e.g. in hip extension/ ankle dorsiflexion etc) |
| 0 | No movement |
| 1 | Flicker of muscle movement |
| 2 | Movement In the plane of gravity |
| 3 | Movement against gravity |
| 4 | Reasonable but reduced power against some resistance |
| 5 | Normal for that person |
Coordination
Check finger –nose testing. Heel to shin movement in lower limbs.
Remember intention tremor of cerebellar disease – (cerebellar signs are ipsilateral i.e. right sided cerebellar problem eg tumour would give right sided intention tremor).
Sensation
Neurotips: Light /fine touch
Dermatomes etc are covered separately: See above classification.
Reflexes
Normal / brisk (UMN)/ reduced(LMN)
Gait
Antalgic/ broad based
Important to just look slick. Do this through practice
The Second Page of the ASIS Standard Classification of Spinal Cord Injury is shown below in figure 2
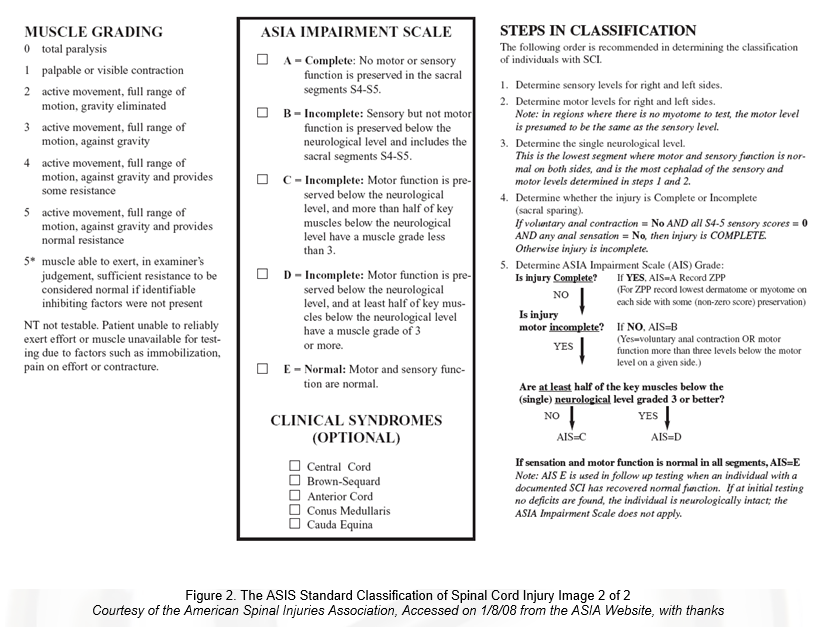
Figure 2. The ASIS Standard Classification of Spinal Cord Injury Image 2 of 2
Courtesy of the American Spinal Injuries Association, Accessed on 1/8/08 from the ASIA Website, with thanks