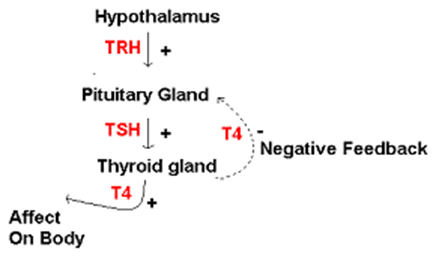
Normal Regulation of Thyroid Hormones:
Thyroid Function tests routinely measure:
- Thyroxine (T4) – hormone that stimulates metabolic pathways, aids cellular differentiation, childhood growth and mental function
- Thyroid Stimulating Hormone (TSH) – hormone released by the anterior pituitary gland that acts on the thyroid gland to stimulate thyroxine production. The pituitary gland can sense the serum level of T4 and adjust production of TSH to maintain a stable level of thyroxine. As a result an increase in the amount of serum T4 reduces production of TSH i.e. negative feedback
Hypothyroidism
- Condition caused by a lack of thyroxine.
- T4 is therefore always low
- TSH is normally high as a result of loss of negative feedback on the anterior pituitary gland
- In the rare instance where hypothyroidism is secondary to pituitary disease (e.g. pituitary infarction in Sheehan’s syndrome or a non-functioning pituitary tumour) both TSH and T4 will be low.
Hyperthyroidism
- Condition caused by an excess of thyroxine
- T4 is therefore always high
- TSH is low as the high T4 suppresses pituitary production of TSH by negative feedback
Investigations
| T4 | TSH | |
| Hyperthyroidism | High | Low |
| Hypothyroidism | Low | High |
| Hypothyroidism secondary to pituitary disease | Low | Low |
Radiological Assessment
Thyroid USS +/- Fine Needle Aspiration (FNA)
- Used to assess goitres or nodules identified on examination.
- If discrete nodules are identified on USS then a FNA is normally carried out to look for malignant cells.
Thoracic inlet CT
- Necessary if a goitre is present with retrosternal extension on examination or if a patient has symptoms suggestive of large goitre e.g. dysphagia, hoarse voice secondary to compression of recurrent laryngeal nerve.
Radioisotope iodine scans
- Radioactive iodine is selectively absorbed by functioning thyroid cells.
- Can be used to assess whether a thyroid nodule is a “hot” functional (i.e. thyroxine producing) nodule or a “cold” non-functional nodule.
- A hot nodule is unlikely to be malignant and is likely to cause hyperthyroidism.
- A cold nodule is likely to be malignant and requires further assessment e.g. by FNA. TSH and T4 levels should be unaffected by a cold nodule.